患者的B肝檢查結果如下:HBsAg(+),Anti-HBsAb(+),HBV DNA:undetectable,這樣要當作有無B肝感染否?
----
先說結論:當作B肝患者隔離。
----
會員們提供的佐證參考資料相當有價值,因此特別記錄下來
1)
The Many Faces of Positive Hepatitis B Surface Antigen
Hepatology. 2016 Oct; 64(4): 1379–1381.
https://aasldpubs.onlinelibrary.wiley.com/doi/full/10.1002/hep.28503
50歲的女性患者要開primary hyperparathyroidism,術前檢查發現如下:
Results of our patient's hepatitis B testing
| Test* | HBsAg** | S/CO*** Ratio | Neutralization Test Result | HBcAb | HBeAg | HBeAb | HBsAb | HBV DNA |
|---|---|---|---|---|---|---|---|---|
| 1 | positive | 3.13 (average 3.07) | non-confirmable | negative | not detected | |||
| 2 | positive | 9.24 | no confirmation necessary | |||||
| 3 | positive | 9.70 | no confirmation necessary | |||||
作者認為可能原因是:Therefore, it is highly suspected that the patient's false positive HBsAg was due to heterophilic interference from a paraneoplastic syndrome related to her parathyroid adenoma.
2)
What are the causes and outcomes of the coexistence of HBsAg and anti-HBs?
Braz J Infect Dis vol.20 no.3 Salvador May./June 2016
http://www.scielo.br/pdf/bjid/v20n3/1413-8670-bjid-20-3-0318.pdf
可能原因:
1. mutations in S gene region, particularly in the ‘a’ determinant.
2. the presence of heterologous subtype-specific antibodies,
3. superinfection with a new (second) hepatitis B virus (HBV) strain,
4. occult HBV reactivation
5. false positivity for anti-HBs (False positivity for anti-HBs may be caused by glycoproteins such as pili fractions isolated from Neiserria gonorrhoeae and Escherichia coli.)
3)
The Interpretation of Diagnostic Blood Tests for Hepatitis B Virus (HBV)
Micropathology Ltd
University of Warwick Science Park, Venture Centre, Sir William Lyons Road, Coventry
# HBV DNA - • May be NOT DETECTED in blood but DETECTABLE in the liver
# Phases of HBV infection: Phase 3: inactive-phase
HBsAg loss and seroconversion to HBsAb may occur spontaneously in ~1.5% of cases per year, usually following several years of undetectable HBV DNA. Patients remain infectious but at a lower level.
4)
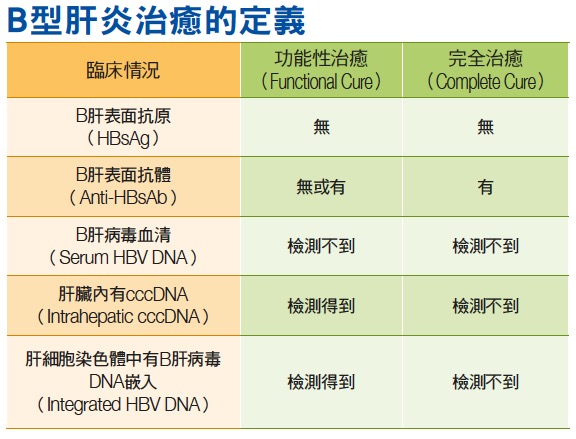
患者的B型肝炎表面抗原消失,但是體內還有具有複製能力的cccDNA存在的情況,被稱為功能性治癒、而非完全治癒。當他們因病情需要接受很強的免疫抑制劑或化療時,比如淋巴癌患者接受化療及莫須瘤(rituximab)治療時,會清除體內大部分的B細胞,統計約有10~15%的人可能因此導致B肝復發,嚴重者甚至出現猛爆型肝炎。因此,這類功能性治癒的B肝患者,雖然血液檢驗看起來不是帶原者,但是當免疫力被抑制時,cccDNA就會再度活化,讓B肝病毒又被製造出來。
財團法人肝病防治學術基金會
https://www.liver.org.tw/newsView.php?cat=3&sid=164
5)

在HBsAg (-) 患者,HBV DNA 占 (+) 57.5%
Investigation of HBV DNA in HBsAg positive patients
Medicine Science 2017;6(4):706-9
https://www.ejmanager.com/mnstemps/53/53-1493293011.pdf?t=1553739690
6)
目前專家意見: B肝分區依據宜以 HBsAg 為準
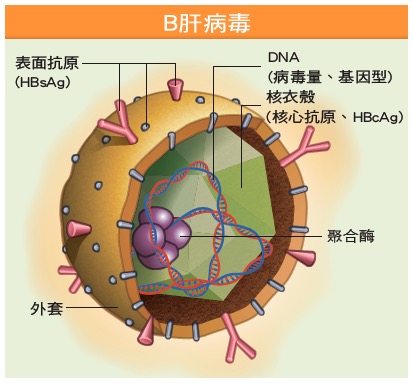
B肝病毒會嵌入肝細胞核之染色體中,即使血中測不到病毒,日後也可能伺機而動。而C肝病毒是在細胞質、不會進入細胞核中,故容易消滅。

7)

沒有留言:
張貼留言